MicSem Publications


Severe Mental Illness in the Federated States of Micronesia: 25 Year Follow-Up of Mental Illness Survey
by Francis X. Hezel, SJ
September 2016 Health
Contents
Introduction
p. 2 – Aims
p. 2 – Methods
p. 3 – Original Data
Findings in Survey
p. 5 – Survival
p. 7 – Drugs
p. 8 – Making Sense of the Drug Use Data
p. 9 – Medical Treatment
References
p. 11 References
Aims
The general purpose of the project was to gather information on the life history over the past 25 years of those 226 persons identified as mentally ill in a 1990 survey of serious mental illness in Micronesia. The information gathered was to show the variations in the course of the illness over time for each individual.
We proposed to analyze the results in terms of personal history of drug use, medical treatment received by patients, the type of care offered in their home environment, the fluctuation in the severity of the symptoms over time, the ability to function in public, correlation to physical ailments, and cause of death.
The goal was to show what types of treatment or general care seem to have proven most beneficial to those who showed improvement over time and, conversely, what factors might have been responsible for worsening the course of their illness.
In the course of the research, we hoped to identify possible subjects for a future, more rigorous study, especially individuals who showed notable improvement or decline over the course of their illness.
Methods
The research team was given access to a database, in the possession of Micronesian Seminar, on serious mental illness gathered over the two-year period 1988-1990. The data include personal life histories on 445 individuals from FSM, Palau and the Marshall Islands who were identified as seriously unstable; 226 of these were from FSM (52 from Yap, 92 from Chuuk, 56 from Pohnpei, and 26 from Kosrae).
This 1990 survey focused exclusively on what is generally regarded as serious mental illness. This included but was not limited to psychoses: “mental disorders in which impairment of mental function has developed to a degree that interferes grossly with insight, ability to meet some ordinary demands of life or to maintain adequate contact with reality” [DSM III, p. 410]. Although the researchers, including the author of this report, had access to the formal psychiatric diagnosis for many of the subjects included in this study, we decided against exclusive reliance on Western medical norms in defining serious mental illness. In determining whether a person for whom we had no formal diagnosis should be regarded as a severely impaired, we adopted a community-based norm. Our field workers asked informants whether the individual had been acting “crazy”–that is, in serious contravention of social norms–at least intermittently, for a period of a year or longer. We excluded from the survey those types of mental illness that were primarily organic in nature, individuals who were impaired from birth or whose problems stemmed from trauma or physical disabilities, and persons who suffer from rather severe but temporary problems.
The project manager of this follow-up study, after copying the database of the original study, examined the mental health files at the FSM Health Office on Pohnpei and then reviewed files on patients at each of the state offices by prearrangement with FSM Mental Health staff. She then gathered additional information on the progress of the individuals listed in the 1990 survey from informed members of the community. The information sought was such as might shed light on the outcome of the illness over the years. We especially noted what general treatment individuals received, the social environment in which they lived, their relationship with their family, changes in the severity of the symptoms over time, compliance with medication prescribed, and the use of other drugs (alcohol, marijuana, etc.) that might have affected the course of their illness. For those who had died in the meantime, we consulted death certificates to find the date, cause and circumstances of death. Any other information that seemed useful was also recorded.
The data, both that from the original survey in 1990 and that obtained during our follow up study, were compiled on a single database and coded. The coded database was then sent off to a consultant, Dr. Jim Anthony at Michigan State University, for analysis by him and his graduate students. Results of the preliminary analysis were sent to the author for compilation in this report.
One of the original 226 SMI cases had died before the 1988 baseline. Hence, this case was set aside for the purpose of the follow up analysis. Consequently, the dataset for the recent follow up includes 225 cases.
Original Data
Table 1: Prevalence of Schizophrenia and Chronic Mental Illness in Micronesia (Adapted from Hezel & Wyllie 1992)
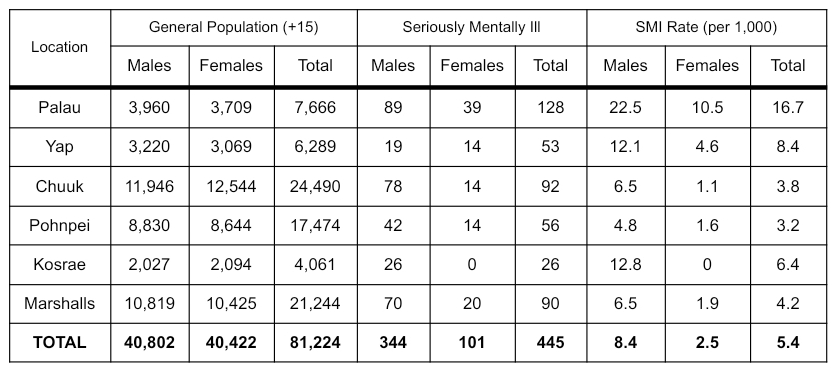
The 1990 survey showed that the general prevalence rates of schizophrenia and chronic mental illness for FSM, while varying from state to state, were within the general range found throughout the globe. As the above table shows, the total rate per thousand people (15 years and older) went from a low of 3.2 in Pohnpei to 8.4 in Yap. The rate of serious mental illness for the whole of FSM was 4.3 per thousand—a rate that falls within the normal range found in other populations (Hezel & Wyllie 1990: 333).
One of the most startling findings in this survey was the great difference in male and female rates, as the table shows. Throughout FSM the male rate was found to be 7 per thousand, while the female rate was given as 1.6. Of the 226 mentally ill found in FSM in 1990, only 43 were females, representing a male-female ratio of 4.3 to 1. This is an unusually high ratio for chronic mental illnesses that are not generally regarded as sex-linked.
Women comprised between 16 to 27 percent of the total psychotic population in each state except Kosrae, where no females were recorded. (It should be noted, however, that Kosrae has had cases of serious mental illness among females in the past.)
Females with schizophrenia and chronic psychosis throughout Micronesia are not only much rarer than males, but they tend to show symptoms of the disease later than males do. The mean age of Micronesian men was about 25 when they first experienced schizophrenia or other mental illness, but women were closer to 30 (Hezel & Wyllie 1992: 342-343). The difference is only six months in Yap, where the average age of onset for males is 28.3 compared to 28.8 for females. In Pohnpei, however, the difference was two years, with an onset age of 25 for males and 27 for females; and in Chuuk, the difference was nearly nine years, with a mean age of 24 for males and 33 for females.
The survey also found that individuals with chronic mental illness in Micronesia were well traveled; “almost half (47 percent) have lived for more than 6 months outside their own state or republic, and most of these have resided on Guam or in the United States” (Hezel & Wyllie 1992: 345-346). The survey report noted, however, that there was no data for the general population against which this could be measured.
Those with serious mental illness were also found to have had a higher level of formal education than the general population. The published report on the survey notes that “the average numbers of years of educational attainment for the adult populations of Yap and Kosrae… are 7.8 and 8.8 respectively. But in our survey, the educational level for people from these areas was 10.1 and 10.7 respectively. The difference is over two years of schooling in Yap and nearly the same in Kosrae…. Nearly one fourth (23 percent) of the subjects surveyed attended college for at least a year, and many spent 2 or 3 years.” (Hezel & Wyllie 1992: 345).
Moreover, the survey found a high incidence of drug use among those with serious mental illness. According to the published report, “88 percent of the males have a history of moderate to heavy drug use, compared with only 36 percent of the females. The most commonly used drug, as might be expected, was alcohol” (Hezel & Wyllie 1992: 343). The data, which include Palau and the Marshalls as well as FSM, are not strong enough to suggest a causal link between psychosis and drug use. Furthermore, the use of drugs might be medicinal as much as causative.
The major finding of the survey–that is, the huge disparity between males and females identified as afflicted with a serious mental disorder–could only be explained tentatively.
Because the genetic predisposition for the major psychoses is not sex linked, as far as we know, the preponderance of males suggests that perhaps environmental factors are responsible. These might include the exposure of males to role changes and other stresses, from which females are better protected by the culture. The sociocultural environment of Micronesia, affected as it has been by modernization and its concomitant changes in recent decades, would appear to be more stressful for many than ever before now. It is conceivable that this could have an effect on the overall rates of psychosis in Micronesia and its distribution among particular segments of these societies. The traditional patterns of social organization in Micronesian cultures tend to shelter women, confining them to the home and keeping them from the public roles that bring men both greater satisfaction and greater stress. Anthropologists who studied Micronesian societies soon after World War ll noted that the social pressures on men were greater and the supports fewer (Gladwin & Sarason, 1953; Lessa, 1951). This should be all the more true today if, as seems to be the case, men are subject to greater role changes and social dislocation than women (Hezel, 1987b).” (Hezel & Wyllie 1992: 348-349)
Findings in Survey
Mortality
Slightly over half (113 of 225) of the mentally ill population had died by the time of this study 25 years later. When the seriously mentally ill population identified at that time is compared with the mortality rate of the general FSM population, we find the death rate of the former about two and a half times greater than the latter. Under normal conditions we might have expected 45 deaths rather than 113, producing a ratio of 2.48 between recorded deaths of the mentally ill and the demographic norm. Mental illness, then, would generally seem to result in an early death for its victims, as the first row in Table 2 indicates.
Table 2: Mortality Rate of FSM Mentally Ill Compared with General Population
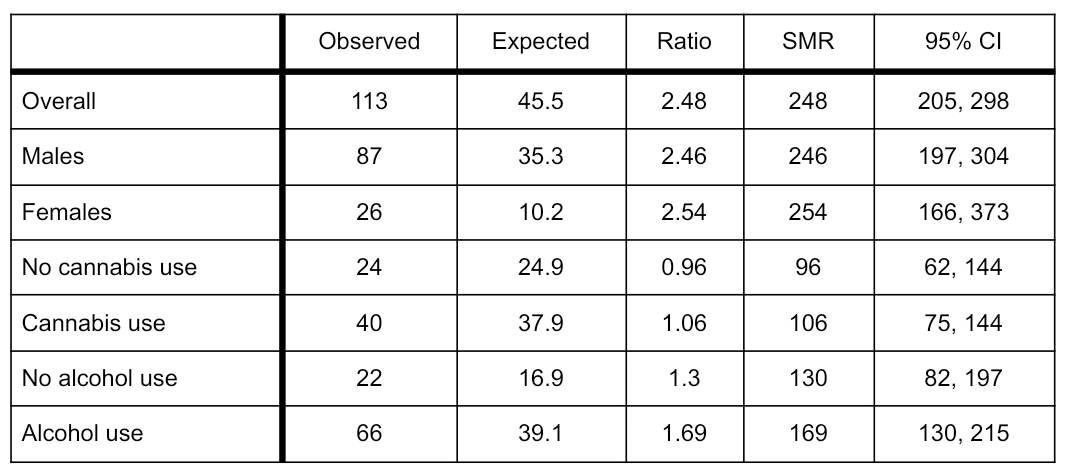
The gap between the mortality rate of the seriously mentally ill and the general population is slightly smaller for males than for females, as the second and third rows in the above table show. The ratio of male deaths among the mentally ill to the general population is 2.46, while that of females is 2.54.
When we ignore the general population and simply compare mortality of males and females within the afflicted population, the difference in mortality appears much more significant. Table 2, which shows mortality by gender since the original survey, brings this out.
Table 3: Fatality Rates among Seriously Mentally Ill in 2015
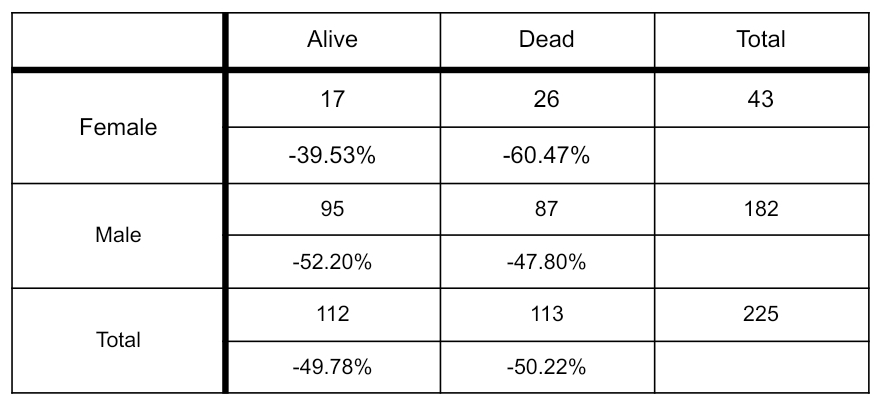
As shown in Table 3, 60% of all female SMI cases died while only 48% of male SMI cases did so. Survival rate for males (52%) is higher than for females (39%). This is surprising inasmuch as in the general FSM population the average life expectancy for females is at least five years higher than for males. Moreover, the males in the survey register a much higher use of drugs than females, which might be expected to put them at still greater risk of death.
The resulting odds ratio estimate from the age-adjusted analysis done supports this finding. The conclusion that female SMI cases in FSM were more likely to die during the observation interval is not contradicted when we use the statistical model to adjust for the male-female age differences (See Figure 1 below).
The survival rate by state varies. Pohnpei had the highest survival rate at 63%, while Kosrae had a survival rate of 54%. Chuuk’s was 46% and Yap’s was 42%. The data gathered and analyzed in the survey was not strong enough to suggest any reason for the differing rates.
Age-specific survival rates for those with serious mental illness are presented in Figure 2. The graph shows that those who were youngest at the time of the original survey had the worst survival rates. Those who were under the age of 35 at the time of the survey show a 15 percent survival rate, low compared with the other age cohorts and the average for the entire caseload. By contrast, those aged 55-74 at the time of the survey show a 60 percent survival rate.
Oddly enough, those who attended high school have a better survival rate than those who did not. The difference is sizable: 57% of those who completed high school are still living, while only 45% of those who did not are still alive. Is this significant? Does it suggest that educational achievement somehow improves survival in the mentally ill? This would be especially odd since in the original survey data, higher educational attainment seems to increase the odds of incurring mental illness in the first place.
Drugs
Alcohol. The great majority (82%) of all those on whom we have information were drinking alcohol before experiencing the onset of mental illness. This is an unusually high rate of alcohol use when we consider that the highest current alcohol use rate in any segment of the general population (males aged 30-44) was 69.5%, according to a survey of alcohol and drug use conducted in 1997 (MicSem 1997: Table 2.7). The comparable rate for the seriously mentally ill, then, is especially high when we consider that the former vary in age and many are women, who normally show a much lower drinking rate.
No notable variation among the states was found, with about 65 to 80% drinking; the one exception was Yap, where over 90% of those with serious mental illness were drinking.
Although the numbers are small, the drinking rate for females with mental illness (43%) was higher than for the general female population (32%).
Drinking after onset of the illness seemed to decrease, if the figures in the follow up survey are reliable. Only 42% of those about whom we have information drank after the onset of the illness; this represents about half the percentage of those using alcohol before onset. Reasons for the decline of alcohol use after illness onset are not clear. We might have thought that the drinking rate would increase, if only because some, especially certain highly visible males, seemed to be using alcohol as medication for their illness.
The mortality rate of SMI alcohol users is higher than for those who have abstained from alcohol. In Table 2, we see that all of the seriously mentally ill have a higher mortality rate than would be found in the general population after adjustments are made for age. The ratio of the mortality age of SMI non-drinkers to the general population is 1.3, while that of SMI alcohol users is 1.69. The difference is not enormous, but it is significant.
Marijuana. The use of marijuana was very high prior to the onset of illness: 74% of those about whom there is information on the subject smoked marijuana (102 of 138). This is a much higher use rate than is registered in the general population. [Even if we use as a denominator 225, the entire case load, still 45% of all patients would have been smoking marijuana before their illness.] No significant difference was noted from state to state. For males, the rate of users would be 85% (96 of 113), and for females 24% (6 of 25).
Cannabis use after the onset of illness, like that of alcohol, declined significantly–55% is the use rate (59 of 108). Of those known to have continued to use the drug after the onset of their illness, however, 73% (43 of 59) are still alive today. So, while the cannabis use rate declined after illness, those who continued to use the drug appeared to have had a much higher survival rate than those who gave up smoking.
Because of the relatively small numbers, it is difficult to compare the mortality rate of cannabis users among the group studied here with the general population. Analysis of the data, presented in Table 2, suggests a negligible difference in mortality rates between those who used cannabis and those who did not. Likewise, Table 2 shows that the impact of cannabis use on mortality within the SMI population is negligible.
Inhalants. Users (15 in all) represent a small number of the total, and the numbers may well be too small to be of statistical significance. Yet, 11 of the 15 known inhalant users are still alive. Only 5 of these (all males) are known to have continued the use of inhalants after the first onset, 4 of whom are still alive today.
Making Sense of the Drug Use Data
The early survey data suggested, even if it could not prove, that the onset of mental illness was very often triggered by drug and alcohol use. Some of the cases were originally diagnosed as genuine schizophrenia or bipolar disorder, while others were diagnosed simply as “drug-related psychosis.” A number of the individuals listed in the original survey had never undergone a medical diagnosis or presented themselves for medical treatment; their abnormal behavior alone had marked them as seriously mentally ill. So frequently did the onset of serious illness seem to follow closely heavy alcohol and drug use that many islanders, including those working in health services, presumed a causal relationship between the two.
The follow up survey that we completed found that many of those who ceased symptoms altogether or at least appeared to be stabilized were often heavy drug users who had stopped taking drugs sometime in the course of their illness. The limitations of our data did not permit us to make any scientific correlations here, but the personal data gathered made a strong case to support some degree of causal relationship..
In Chuuk, 14 of the 41 individuals who were still alive at the time of the follow up had shown marked improvement, according to the medical files and personal reports. In nearly all of the cases reported, the individual had given up drug use. In some cases a dramatic improvement was noted, while in others the individual was simply reported as having been “stabilized.” In Kosrae, eight of the 14 still alive showed notable improvement, most of them to the point where they exhibited none of the former symptoms. Five of these were said to have given up all use of drugs prior to their improvement. Yap and Pohnpei did not show the same dramatic numbers as the other two states. Yap had three persons reported as showing significant stabilization, while Pohnpei had four. In only one case of those from Yap and Pohnpei could the improvement be linked with the cessation of drug use.
Overall, several of these individuals showed such improvement that they married and held down regular jobs. Thus, the case reports contain strong evidence that the cessation of drug use often results in attenuation of symptoms and stabilization, even though drug and alcohol users appear statistically to live longer lives. Clearly, additional research needs to be done on this matter.
Medical Treatment
The database included many individuals who received professional medical treatment but others who did not. As the following graph shows, treatment seems to be associated with reduced mortality, at least for males. The survival rate is about 15 percent higher for those who underwent treatment during their illness.
Apart from higher survival rates, is there evidence that medical treatment is associated with a better outcome for patients? The data suggest some improvement in the case of females, since the symptoms may be less severe in those women who have undergone treatment; but the correlation is not strong enough to be compelling. There is little statistical evidence for an association in the case of males, though.
A careful look through the case reports suggests that improvement will frequently occur when the person maintains strong ties with his or her own family. Of course, the family will invariably encourage its mentally sick member to abstain from drugs and to take the prescribed medication. In the case files may be found the accounts of three young men from different coral atolls who showed notable improvement after their communities rallied around them and provided a high level of support. This merely suggests the obvious: that strong support from the family and community might be one of the most important factors in achieving improvement in the seriously mentally ill. It might prove to be at least as important as compliance with official medical treatment offered.
References
Dale, P. W. (1981). Prevalence of schizophrenia in the Paciflc Island populations of Micronesia. Journal of Psychiatric Research, 16, 103-111.
Gladwin, T., & Sarason, S. (1953). Truk. Man in paradise. Viking Fund Publications in Anthropology, No. 20. New York: Wenner-Gren Foundation.
Hezel, F. X. (1987a). In search of the social roots of mental health pathology in Micronesia. In A. Robillard & A. Marsella (Eds.), Contemporary issues in mental health research in the Pacific Islands (pp. 12-31). Honolulu: University of Hawai’i Press.
Hezel, F. X. (1987b). The dilemmas of development: The effects of modernization on three areas of island life. In S. Stratigos & P. Hughes (Eds.), The ethics of development: The Pacific in the 21st Century (pp. 60-74). Port Moresby: UPNG Press.
Hezel, F.X., and Wyllie, M. (1992). Schizophrenia and Chronic Mental Illness in Micronesia: An Epidemiological Survey. Isla,1.2, (1992), 329-354.
Lessa, W. A. (1951). The Ethnography of Ulithi Atoll. Unpublished doctoral dissertation, University of California, Los Angeles.
Micronesian Seminar. (1997). Alcohol and Drug Use in the FSM. Pohnpei, FSM: Francis X. Hezel, S.J.